Indoor air is full of flu and COVID viruses
March 8th, 2023
The current pandemic has focused attention to the importance of healthy indoor air and could spur lasting improvements to the air we breathe.
Article from Nature by: Dyani Lewis
Bars in Belgium could be among the healthiest places to have a drink, come July. That’s when a new law goes into effect, requiring public venues to meet air-quality targets and display real-time measurements of carbon dioxide concentrations — a proxy for how much clean air is piped in.
Consumers in Belgium will get even more information in 2025, when gyms, restaurants and indoor workspaces must all show air-quality ratings given through a certification system. In the event of a future pandemic, Belgium’s rating system could determine whether or not a venue is closed.
The law, enacted in July 2022, is the boldest in a string of moves that countries have taken in the wake of the COVID-19 pandemic to make indoor spaces safer in the face of infectious diseases caused by viruses such as SARS-CoV-2 and influenza.
In March 2022, the US government launched a Clean Air in Buildings Challenge to spur building owners and operators to improve their ventilation and indoor air quality. In October last year, the state of California passed a law requiring all school buildings to provide clean indoor air. And in December, the White House announced that all federal buildings — some 1,500 in total — would meet minimum air-safety requirements. Also in December, the American Society of Heating, Refrigerating and Air Conditioning Engineers (ASHRAE) — a construction-industry body whose recommendations are adopted into law through local building codes in the United States and elsewhere — announced that it would be developing standards that take infection risk into account by June 2023.
Last June, the United Kingdom’s leading engineering bodies released a report, commissioned by the government, that called for enforceable clean-air regulations to make buildings safe over their entire lifetimes (see go.nature.com/3kgsmjt). Other countries are also taking steps — for example, by deploying air-quality monitors in classrooms.
Specialists in indoor air quality are buoyed by the prospect that the pandemic could bring lasting improvements to the air we breathe indoors. The SARS-CoV-2 virus that causes COVID-19 is spread mainly in indoor spaces, as are the pathogens that lead to other infectious diseases, such as chicken pox, measles, tuberculosis and seasonal influenza.
“There’s never been, in history, so much action about indoor air quality,” says Lidia Morawska, an aerosol scientist at the Queensland University of Technology in Brisbane, Australia.
But huge challenges lie ahead, particularly for the existing stock of schools, office buildings and other public venues. Retrofitting them with the technology to deliver clean air at sufficient levels will be an immense — and costly — undertaking, say experts in this field. But, they argue, the benefits would outweigh the costs. By one estimate, pandemic and seasonal influenza outbreaks cost the United Kingdom £23 billion (US$27 billion) per year, on average (see ‘The high cost of outbreaks’), and the country could save £174 billion over a 60-year period by improving ventilation in buildings (see go.nature.com/3ktumeg).
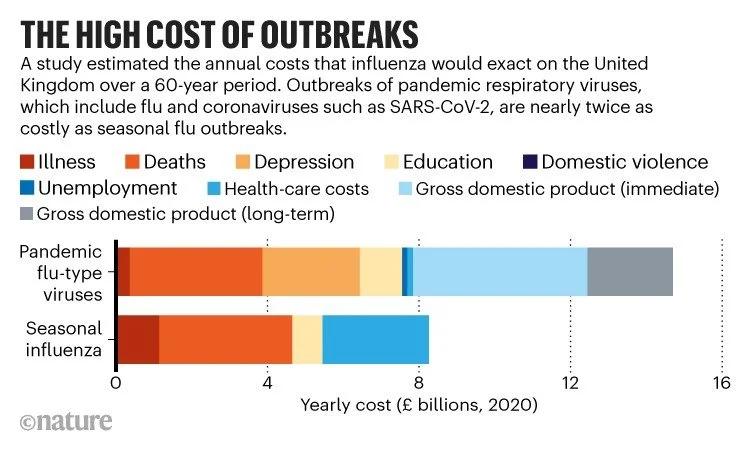
Source: NERA Economic Consulting
Making indoor spaces safe from infection could also reduce exposure to pollutants such as fine particulates from wildfire smoke and cooking, volatile organic compounds leached from furniture, and allergy-causing moulds and pollen. But it could also raise energy costs and contribute to greenhouse-gas emissions.
Researchers are still working to pin down how best to ventilate indoor spaces to prevent infections from spreading, and what alternative technologies might replace or enhance mechanical ventilation systems. But many say that enough is already known to start demanding safer indoor spaces.
It’s a race against time. As concern over COVID-19 wanes, experts wonder how much progress countries will make before the next big outbreak of an airborne infectious disease.
Reducing infections
When COVID-19 reached pandemic status in early 2020, health officials didn’t pay much attention to the risks of indoor air. Initially, the World Health Organization (WHO) dismissed the role of airborne transmission and focused — incorrectly — on transmission through contaminated surfaces. But even when public-health authorities began recommending better ventilation as a way of preventing infection, they offered only vague guidance. Authorities told people to open windows and bring in as much outdoor air as possible with mechanical ventilation systems, without giving specific numbers.
Such advice sowed confusion, says Joseph Allen, a building hygienist at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts. “You can’t tell people to bring in more outdoor air without answering how much,” he says.
Allen was one of the first to put a value on how much ventilation people should be aiming for. In June 2020, he and his colleagues recommended that schools wanting to reopen their doors after lockdowns should deliver four to six air changes per hour to their classrooms1 — changes in which the entire volume of air in the room is replaced. That amounts to a ventilation rate of 10–14 litres per second per person. Most schools were achieving much less than that, however. A study of California classrooms, for example, found that most failed to meet that level of ventilation2. The WHO issued its own guidelines in March 2021, recommending a ventilation rate of 10 litres per second per person outside health-care settings.
In theory, the pandemic provided the perfect opportunity to gather real-world data to see whether low ventilation rates were associated with outbreaks, and to test different rates of ventilation to see which resulted in reduced infection rates. But health officials only rarely considered ventilation when investigating major outbreaks of COVID-19. Yuguo Li, a mechanical engineer at the University of Hong Kong, estimates that fewer than ten investigations measured ventilation rates in venues where outbreaks occurred, because airborne transmission was not on people’s radar.
Instead, researchers tried to gain clues through observational studies. Morawska was involved in one that looked at 10,000 school classrooms in the Marche region of Italy. In the 316 classrooms that had mechanical ventilation with rates of 1.4–14 litres per second per person, the students’ risk of infection was reduced by at least 74% over a 4-month period at the end of 2021, compared with that for students in classrooms that relied on windows for ventilation. This group typically received less than 1 litre per second per person. When ventilation rates were at least 10 litres per second per student, the infection risk was 80% lower3.
Evidence is also growing about other technologies that remove infectious particles from the air. One study4 explored the effectiveness of two air cleaners fitted with high-efficiency particulate absorbing (HEPA) filters, placed in a 54-square-metre conference room with a dummy that generated aerosol particles similar to those that transmit SARS-CoV-2. The cleaners reduced the aerosol exposure of three dummy participants by 65%. That’s just shy of the 72% reduction achieved by masking all of the dummy participants4.
Another study, by civil engineer Bert Blocken at the Catholic University of Leuven (KU Leuven) in Belgium, found that ventilation combined with air cleaning, equivalent to 6 air changes per hour in total, reduced exhaled aerosol concentrations in a gym to 5–10% of what they would have been without these measures5. That concentration substantially reduces infection risk, says Blocken. He adds that air cleaners are an underappreciated technology that could be readily deployed in buildings that don’t have mechanical ventilation systems capable of providing enough clean air, or where operating such systems would consume too much energy. The state of Victoria in Australia took this approach, distributing portable air cleaners to all of its 110,000 classrooms in 2022.
Last November, the Lancet COVID-19 Commission’s Task Force on Safe Work, Safe School, and Safe Travel, chaired by Allen, published concrete guidelines for clean-air delivery rates — using ventilation, air filtration or other means — to reduce airborne infections6. To achieve what the report describes as the ‘best’ air quality, it recommends more than 6 air changes per hour, or 14 litres per second per person (see ‘How much clean air is enough?’).
How much clean air is enough?
A task force of researchers proposed ventilation rates for buildings using several metrics*, with the aim of reducing the risks of transmission of airborne respiratory diseases.

*Not shown: volumetric flow rates per floor area.
Legal limits
Ventilation requirements can be complicated, because they change depending on how big the space is, how many people are in it and how active they are. So some researchers advocate using a shortcut — setting maximum carbon dioxide concentrations. CO2 is frequently used as a proxy measure for ventilation and indoor air quality7. Because people exhale CO2 as they breathe, levels of the gas can shoot up if a space is crowded or if there is insufficient ventilation to replace the exhaled air — which might contain infectious viruses — with clean air.
Until 1999, ASHRAE standards included a recommended limit for CO2 of 1,000 parts per million (p.p.m.). At this concentration, according to research conducted in the 1930s, building occupants’ perception of body odour would be kept at an acceptable level. Since then, research has shown that when concentrations exceed 1,000 p.p.m., CO2 can cause drowsiness and can impair cognitive performance on decision-making and problem-solving tasks8.
A small study published in September 2022 — and yet to be peer reviewed — directly connected CO2 levels with those of infectious pathogens. The authors tested air samples in nurseries, schools, universities and care homes for the presence of respiratory pathogens. Rooms that had higher CO2 levels were associated with higher levels of respiratory pathogens9.
In August 2021, the UK government began distributing CO2 sensors to all school classrooms so that teachers could use the devices to decide when to open windows or increase ventilation. Similar schemes have been rolled out in Europe, the United States and elsewhere, although none has yet been evaluated for its ability to reduce infection rates.
Relying on CO2 readings has drawbacks, however. Concentrations can creep up even when the infection risk remains low, such as when using portable air cleaners — which do not remove CO2 from the air — or when cooking. CO2 is useful, says chemist Nicola Carslaw at the University of York, UK, who studies indoor-air pollutants, “but it’s definitely not the whole story”.
Despite these issues, Morawska says that CO2 monitors should be widely deployed as an inexpensive, readily available tool that could be installed in every indoor space, much like smoke alarms. But displaying CO2 read-outs on its own is not enough, she adds, because it places the onus on room occupants to track air quality and decide what to do if readings are high.
Morawska would also like to see laws that mandate maximum CO2 levels permissible in public buildings, so that the responsibility is placed back on building operators and government regulators. A handful of governments have already done just that. Last year, Morawska and her colleague Wei Huang at Peking University in Beijing reviewed air-quality laws in more than 100 countries. Only 12 had national standards for indoor air quality that specified threshold limits for pollutants. And only 8 of those — including China, South Korea, India, Poland and Hungary — set limits for CO2 concentration, most between 800 p.p.m. and 1,000 p.p.m.10.
Japan has had a law to regulate indoor air quality since 1970, which mandates that buildings must not exceed indoor CO2 concentrations of 1,000 p.p.m.. The law requires that building managers assess air quality every two months, report results to the government and establish remediation plans if the air quality does not meet the standards. But almost 30% of buildings exceeded the CO2 limit in 2017, according to a 2020 report11.
Still, the Japanese laws work, says Kazukiyo Kumagai, a public-health engineer at the California Department of Health in Richmond. “Japan is in a better condition” than the United States when it comes to indoor air quality, he says. Adopting a Japanese-style approach of regular monitoring and reporting might work elsewhere, he adds.
Legal limits could become more common. The new Belgian law, for example, comes into effect in July this year and stipulates that public venues ventilate at a rate of 40 cubic metres per hour so that CO2 does not exceed 900 p.p.m.. If air filtration is used, a lower ventilation rate of 25 cubic metres per hour is enough, and CO2 can reach a maximum level of 1,200 p.p.m..
Legislating indoor air quality is “tricky” says Catherine Noakes, a mechanical engineer at the University of Leeds, UK, who contributed to that country’s report into infection-resilient buildings. “One of the challenges with indoor air,” she says, “is who owns it?” The responsibility can be distributed across government departments and agencies, depending on how the building is used. A school’s indoor air might be the responsibility of the education department, whereas office buildings could be regulated by an occupational health and safety agency.
That’s the situation in the United States, where no agency currently has the authority to regulate indoor air, says Andrew Persily, a mechanical engineer at the National Institute of Standards and Technology in Gaithersburg, Maryland. In Belgium, too, the new national law doesn’t cover schools, which are the responsibility of regional governments. And in Japan, a separate law for school buildings specifies a higher CO2 limit of 1,500 p.p.m., a level many regard as too high.
Setting standards
In the absence of national laws, professional bodies that set air-quality standards are starting to act. When ASHRAE releases its infection-mitigation standard in June, the hope is that these recommended targets will be adopted into local building codes that new buildings must comply with.
“We have always addressed indoor air quality, but not specifically for pathogen mitigation,” says engineer Ginger Scoggins, the president-elect of ASHRAE, who is based in North Carolina. ASHRAE could face some pushback. Scoggins says that when the society made a previous change to increase the ventilation requirement from 5 cubic feet per minute to 15 (2.4 litres per second to 7.1 litres per second), many people in the warm parts of the United States were angry because it would drive up energy costs from air conditioning. Her local school board passed a ruling that its classrooms only needed to get to 7.5.
Even though ASHRAE standards are not enforced, they will make a difference, says Allen. Aside from influencing how buildings are constructed, more stringent ASHRAE standards send a strong signal to businesses in older buildings about what the gold standard for indoor air quality looks like.
An economic case could be made for better indoor air, says Noakes. The cost–benefit analysis conducted for the UK report found that the country could save £3 billion per year over a 60-year period by improving ventilation.
Researchers say it will take time to lower the infection risks inside buildings. “We are looking at 30 years,” says Morawska. “But we are talking about the future of our society.”
[Source: Nature 615, 206-208 (2023)]